What Is Periodontal Disease?
Periodontal disease is a chronic bacterial infection that damages the structures supporting your teeth, including your gums, the periodontal ligament, and most importantly, the jawbone that holds your teeth in place. Unlike a cavity, periodontal disease destroys the foundation rather than the tooth itself. The damage is caused by your immune system's inflammatory response to persistent bacteria, and once bone is lost, it does not grow back on its own.
Key factors that influence the disease include:
- Bacterial biofilm – Hardened plaque (calculus) shields bacteria from antibiotics and requires physical removal
- Your immune response – Inflammation that protects you can also become destructive when bacteria persist
- Local anatomy – Tooth position, bone thickness, and furcations affect how the disease progresses
- Systemic health – Conditions like diabetes, smoking, and stress can accelerate bone loss
For a comprehensive understanding of what causes periodontal disease, how it progresses, and how it affects your overall health, read our full article: Understanding Periodontal Disease.
How Your Treatment Works
Treating periodontal disease is not a single appointment; it is a carefully planned sequence of steps, each building on the results of the last. This phased approach is supported by decades of clinical research and is recommended by the European Federation of Periodontology's official treatment guidelines.
Phase One: Scaling and Root Planing (Your Deep Cleaning)
Why This Is Always the First Step
Scaling and root planing (SRP) is the foundation of periodontal treatment and is performed before any other intervention, regardless of how advanced your disease may be. Even if you ultimately need surgery, deep cleaning is always done first, and for very good reasons.
The primary purpose is to physically remove the bacterial biofilm, hardened tartar (calculus), and bacterial toxins from the root surfaces of your teeth below the gum line. By removing the source of infection, we give your body the chance to begin healing.
For patients who will eventually need surgery, performing deep cleaning first is critical because it significantly reduces inflammation in the gum tissue. When surgery is performed on highly inflamed tissue, the gums tear easily, the procedure takes longer, healing is more painful, and results are worse. By controlling inflammation first, we ensure surgery goes as smoothly as possible with the best outcome. Additionally, some patients heal better from deep cleaning than we expect, and sites that seemed to need surgery may actually resolve without it.
What Happens During the Procedure
Your mouth will be numbed with local anesthesia so you are completely comfortable throughout. Treatment is typically done one section of your mouth at a time (either by quadrant or by half).
Your hygienist or periodontist will use a combination of two types of instruments:
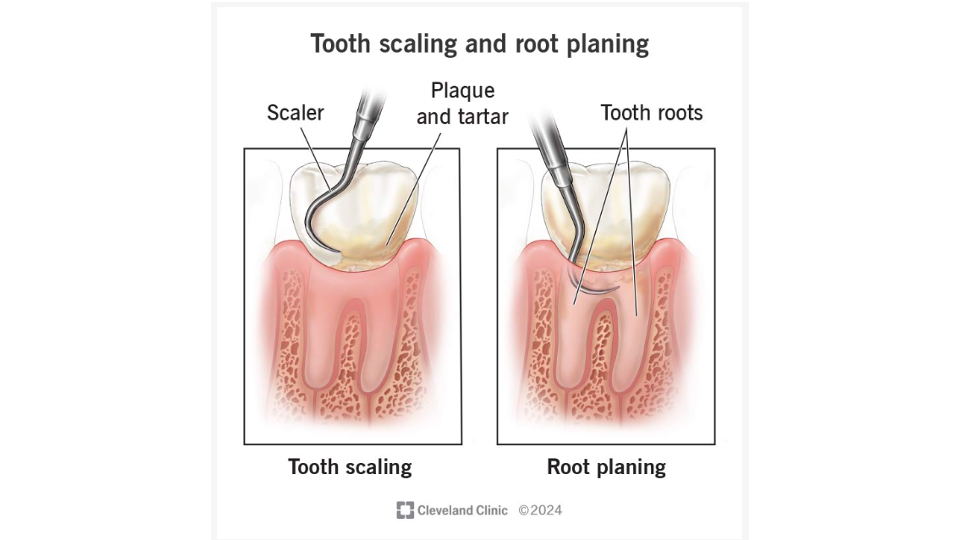
- Ultrasonic scalers use high-frequency vibrations to break apart and dislodge hardened tartar deposits while simultaneously flushing debris from the pocket with a stream of water.
- Hand instruments (called curettes) are then used to carefully smooth each root surface, removing remaining tartar and the bacterial toxins that have soaked into the root.
The goal is to create a clean, smooth surface that your body recognizes as healthy, allowing gum tissue to heal and potentially reattach to the root.
In deeper pockets (6 mm or greater), reaching every surface becomes increasingly difficult due to limited access and complex root anatomy. This is one of the reasons deeper sites sometimes need surgical treatment after healing, so we can gain the direct visibility that closed instrumentation cannot provide.
How Healing Works After Deep Cleaning
Healing happens in two phases:
- First two weeks: Inflammation subsides; you will notice your gums looking less red and puffy, and bleeding will decrease.
- Two to six weeks: If enough bacteria were removed, the gum tissue can actually reattach to the root surface, reducing your pocket depths.
What Results Can You Expect?
- Starting pockets of 4 to 5 mm: Research shows that deep cleaning typically reduces these pockets by 1 to 2 mm, with about 0.5 to 1.0 mm of tissue reattachment. In most cases, these sites resolve to a healthy, maintainable range and surgery is not needed.
- Starting pockets of 6 mm or deeper: Deep cleaning typically achieves 2 to 3 mm of reduction, but pockets often remain at 4 to 6 mm or deeper. When this happens, surgical treatment is usually needed to fully address the remaining disease.
Adjunctive Laser Therapy
Why We Recommend Laser
While deep cleaning is highly effective at removing bacteria from root surfaces and the pocket space, it has one fundamental limitation: it cannot reach bacteria that have invaded your gum tissue itself. Aggressive bacteria like P. gingivalis can penetrate into the cells of your gum tissue, creating hidden reservoirs of infection that mechanical cleaning alone cannot eliminate. Laser therapy addresses this gap.
How the Laser Works
The lasers used in periodontal treatment (typically diode lasers operating at 810 to 980 nm wavelength) deliver focused light energy that is absorbed by pigmented, inflamed, and bacteria-laden tissue. This energy works in several important ways:
- Kills bacteria: Both in the pocket and within the tissue. The laser energy penetrates 1 to 3 mm into gum tissue, generating heat that destroys bacteria hiding inside tissue cells.
- Removes diseased tissue: The laser removes the infected, ulcerated lining of the pocket, eliminating a source of ongoing inflammation and creating conditions for healthy new tissue to form.
- Stimulates healing: At lower energy levels, laser light stimulates your cells to heal faster (photobiomodulation). It promotes new connective tissue cell growth, encourages new blood vessel formation, and shifts the chemical environment from inflammation toward repair.
- Controls bleeding: The heat seals blood vessels in the treated area, reducing bleeding and helping to stabilize the blood clot essential for wound healing.
When Laser Is Recommended
We recommend laser therapy for all patients showing signs of active inflammation (bleeding on probing) and those with evidence of high levels of pathogenic bacteria. The laser is used immediately after mechanical cleaning at each treated site, adding minimal time and discomfort to your appointment.
Subgingival Irrigation
Why Irrigation Matters
Even with the most thorough deep cleaning, it is physically impossible to remove 100% of bacteria from deep periodontal pockets, especially in areas with complex root anatomy, furcation involvement, or winding pocket shapes. Subgingival irrigation provides two additional benefits: it physically flushes out dislodged bacterial debris, and the antimicrobial solution provides chemical disinfection of the pocket.
What Solutions Are Used
- Chlorhexidine gluconate (0.12 to 0.2%): The gold standard antimicrobial rinse in dentistry. It provides broad-spectrum bacterial killing and has "substantivity," meaning it binds to surfaces in the pocket and continues providing antimicrobial protection for 8 to 12 hours.
- Povidone-iodine: Especially effective in aggressive disease.
- Dilute sodium hypochlorite: An excellent biofilm disruptor.
- Stannous fluoride solutions: Also help with tooth sensitivity.
How It Is Performed
Using a blunt-tipped syringe or an ultrasonic scaler with built-in irrigation, the antimicrobial solution is delivered directly to the base of each treated pocket under gentle pressure. This is performed after both mechanical cleaning and laser therapy, creating a three-layer approach (mechanical removal, laser disinfection, chemical irrigation) that represents the current best-practice standard for non-surgical periodontal treatment.
The Re-Evaluation: Your Progress Check
Between four and eight weeks after your deep cleaning is completed, you will return for a comprehensive re-evaluation. This is one of the most important appointments in your entire treatment. We will re-measure every pocket, check for bleeding, and compare results to your baseline numbers.
What Your Re-Evaluation Numbers Mean
- Pockets at 1 to 3 mm, no bleeding: Excellent! These sites have fully resolved. They enter maintenance and need no further active treatment.
- Pockets at 4 to 5 mm, no bleeding: These sites are stable but still at some risk. We will monitor them closely at every cleaning appointment.
- Pockets at 5 mm with bleeding: The bleeding tells us active inflammation persists. These sites are indicated for surgery because non-surgical treatment has not fully controlled the disease.
- Pockets at 6 mm or deeper: These sites have craters in the bone that are preventing complete healing. Surgery is needed to access these areas and correct the bone architecture.
Phase Two: Osseous Surgery
What Is Osseous Surgery?
Osseous surgery, sometimes called periodontal flap surgery, is the definitive surgical treatment for periodontal disease that has not fully responded to deep cleaning. Think of it as a "surgical deep cleaning": by gently lifting the gum tissue, Dr. Yant gains direct access to see and clean every root surface and bone defect that was hidden during the non-surgical phase.
The goals are threefold:
- Completely remove all remaining bacteria and tartar that could not be reached during deep cleaning
- Correct the pathological bone shapes (craters, ledges, defects) that are preventing healing and trapping bacteria
- Where appropriate, rebuild lost bone support through grafting
Before Your Surgery
Successful surgery starts with preparation. You must have completed your deep cleaning and be demonstrating good oral hygiene at home. We will review your medical history carefully. If you have diabetes, we want your HbA1c below 7%. If you smoke, we strongly encourage you to quit before surgery; smokers have significantly higher rates of complications and poorer long-term results.
What Happens During Surgery
Anesthesia and access: The surgical area is thoroughly numbed. Precise incisions are made along the gum tissue, and the gums are gently lifted away from the bone to expose root surfaces and underlying bone defects. This direct visualization is the critical advantage of surgery: Dr. Yant can now see everything that was previously hidden.
Root surface debridement: With full visibility, every remaining trace of tartar, contaminated root material, and bacterial biofilm is meticulously removed. The chronically inflamed tissue filling bone defects (granulation tissue) is also removed. This is far more thorough than anything achievable with closed treatment, because the surgeon can visually confirm that every surface is completely clean.
Correcting the Bone: Reshaping vs. Rebuilding
In a healthy mouth, bone around your teeth has a smooth, peaked shape, like mountain peaks between each tooth. Periodontal disease changes this shape, creating craters, ledges, and defects. Treatment depends on the shape and depth of each defect.
Bone reshaping (resective surgery): When craters are shallow to moderate, bone is carefully reshaped to recreate the healthy "mountain peak" form. This may involve smoothing the outer bone surface and, when necessary, removing small amounts of bone to eliminate crater walls. The guiding principle is always to remove the minimum bone necessary to achieve a healthy architecture.
Graphic Image Warning
These images contain clinical dental photography showing before and after osseous surgery
Graphic Image Warning
These images contain clinical dental photography including surgical images
Bone grafting (regenerative surgery): When defects are deep and well-contained (meaning several walls of bone still surround the defect), we can actually rebuild lost bone. Bone graft material is placed into the defect to serve as a scaffold that your body uses to grow new bone. The material may be processed human donor bone, bovine-derived mineral, or synthetic biocompatible material.
A barrier membrane may be placed over the graft. This membrane acts like a protective tent, preventing fast-growing gum cells from filling the space before the slower-growing bone cells have time to regenerate. Biologic proteins (such as enamel matrix derivative or growth factors) may also be applied to enhance regeneration.
Graphic Image Warning
These images contain clinical dental photography showing bone regeneration procedure steps
Often, your surgeon will use both approaches within the same procedure, reshaping shallow defects on some teeth and grafting deep defects on others. This customized, tooth-by-tooth approach reflects the precision of modern periodontal surgery.
After Your Surgery
You will receive detailed post-operative instructions. During the first 7 to 14 days, you will:
- Avoid brushing the surgical area
- Rinse gently with chlorhexidine twice daily
- Eat a soft diet
- Avoid smoking and alcohol
- Sutures are typically removed at 7 to 14 days
It is normal for gum tissue to sit lower on your teeth after surgery. This happens because resolving deep pockets involves the gums tightening and repositioning closer to the bone. While this may result in some additional tooth exposure, it is an expected and necessary trade-off for achieving the healthy pocket depths that will protect your teeth long-term.
What Does the Research Say About Outcomes?
The evidence supporting osseous surgery is extensive and encouraging:
- For sites starting at 7 mm or deeper, surgery typically achieves 3 to 4 mm of pocket reduction with significant tissue attachment gains.
- Long-term comparative studies show surgery produces better results than deep cleaning alone at sites with initial depths over 6 mm.
- Regenerative procedures in well-suited defects achieve average attachment gains of 3 to 4 mm and radiographic bone fill of 2 to 3 mm.
- When pockets are successfully reduced to 1 to 3 mm, studies with 15 to 20 years of follow-up show tooth retention rates exceeding 90% in patients who maintain their cleaning schedule.
Lifelong Maintenance: The Key to Keeping Your Results
After active treatment is complete, you enter the most important phase: supportive periodontal therapy. This is your long-term maintenance program and it is what protects the investment you have made in your oral health.
You will need professional cleanings every three months (sometimes every two). Each visit includes:
- A comprehensive re-examination of all pocket depths and bleeding points
- Professional cleaning above and below the gum line
- Assessment of your oral hygiene with coaching on any areas needing attention
- Evaluation of changes in your overall health that might affect your periodontal status
Why Three Months? Why Not Every Six Months?
Periodontal disease is a chronic condition. The genetic and immunological susceptibility that led to your bone loss in the first place does not change after treatment; it must be continuously managed. Research consistently shows that patients who keep to their maintenance schedule have dramatically lower rates of tooth loss, disease recurrence, and need for retreatment compared to patients who are inconsistent. Think of it like managing any chronic condition: the treatment brings the disease under control, and maintenance keeps it there.
What You Can Control
While many factors in periodontal disease are beyond your control, there are powerful things you can do to improve your outcome at every stage:
Oral hygiene is number one. Brush twice daily with a soft-bristled toothbrush, making sure to angle the bristles at the gum line. Clean between your teeth every day, with floss, a water flosser, or ideally an interproximal brush (a small brush that looks like a tiny pipe cleaner and is especially effective when gaps between teeth have widened due to periodontal disease). Choose the largest size that fits comfortably. You can rinse and reuse these brushes as long as the bristles remain straight.
If you smoke or vape, please consider quitting. Nicotine in any form constricts blood vessels in your gums, weakens your immune response, impairs tissue healing, and significantly increases your risk of treatment failure and tooth loss.
If you have diabetes, work with your doctor to optimize your blood sugar. An HbA1c below 7% gives you the best chance of successful healing.
Keep every maintenance appointment. This is not optional. Your three-month cleanings are a medical necessity, not a convenience. Patients who maintain their schedule keep their teeth. Patients who skip appointments lose them.
A Final Word
Periodontal disease is a serious condition, but it is not a hopeless one. Modern periodontal treatment, following the phased approach outlined in this guide, gives you a clear, proven pathway from active disease to long-term stability. When scaling and root planing is augmented with laser therapy and antimicrobial irrigation, and when osseous surgery is performed where needed with the appropriate resective or regenerative techniques, the results are excellent.
Research with 15 to 20 years of follow-up shows that patients who complete treatment and commit to maintenance can expect to keep their teeth for decades. The key is partnership between you and your periodontal care team, and it begins with the decision to move forward with treatment.
We are here to support you at every step.
Frequently Asked Questions
What happens at a periodontal consultation?
At your first visit, the periodontist will review your medical and dental history, take X-rays, measure the depth of the pockets around your teeth, and assess the health of your gums and bone. You will receive a diagnosis and a recommended treatment plan before any treatment begins.
Do I need gum surgery?
Not everyone with gum disease needs surgery. Many cases can be managed with deep cleaning (scaling and root planing) and improved home care. Surgery is typically recommended when pockets are too deep to clean effectively with non-surgical methods, or when bone loss requires correction.
What is scaling and root planing?
Scaling and root planing is a non-surgical deep cleaning performed under local anesthesia. Scaling removes plaque and tartar from above and below the gum line. Root planing smooths the root surfaces so the gums can reattach more tightly to the teeth. Most patients need two to four visits to complete treatment.
How long does periodontal treatment take from start to finish?
The timeline depends on the severity of your condition. A typical course of treatment begins with deep cleaning, followed by a healing period of 6 to 8 weeks, then a reevaluation. If surgery is needed, that adds additional time. From first appointment to stable maintenance, most patients are looking at 3 to 6 months.
What is periodontal maintenance and how often do I need it?
Periodontal maintenance is a specialized cleaning performed every 3 to 4 months after active treatment. It is more thorough than a standard dental cleaning and focuses on keeping bacteria under control in areas where disease was previously active. Consistent maintenance is essential to prevent recurrence.
What is the difference between a periodontist and a dentist?
A periodontist is a dentist who has completed an additional 3 years of specialized training in the treatment of gum disease, bone loss, and dental implant placement. Your general dentist handles routine care, while a periodontist manages complex periodontal conditions that require advanced expertise.
Sources
This guide is based on peer-reviewed research published in leading dental and medical journals.
- Aoki, A., Sasaki, K. M., Watanabe, H., & Ishikawa, I. (2004). Lasers in nonsurgical periodontal therapy. Periodontology 2000, 36, 59-97.
- Bergstrom, J. (2004). Tobacco smoking and chronic destructive periodontal disease. Odontology, 92(1), 1-8.
- Cobb, C. M. (2002). Clinical significance of non-surgical periodontal therapy: an evidence-based perspective of scaling and root planing. Journal of Clinical Periodontology, 29(Suppl. 2), 6-16.
- Cobb, C. M., Low, S. B., & Coluzzi, D. J. (2010). Lasers and the treatment of chronic periodontitis. Dental Clinics of North America, 54(1), 35-53.
- Cortellini, P., & Tonetti, M. S. (2011). Clinical and radiographic outcomes of the modified minimally invasive surgical technique. Journal of Clinical Periodontology, 38(4), 365-373.
- Drisko, C. H. (2001). Nonsurgical periodontal therapy. Periodontology 2000, 25, 77-88.
- Greenstein, G. (2000). Nonsurgical periodontal therapy in 2000: a literature review. Journal of the American Dental Association, 131(11), 1580-1592.
- Heitz-Mayfield, L. J., et al. (2002). Systematic review of surgical debridement vs non-surgical debridement for chronic periodontitis. Journal of Clinical Periodontology, 29(Suppl. 3), 92-102.
- Herrera, D., Matesanz, P., Bascones-Martinez, A., & Sanz, M. (2012). Local and systemic antimicrobial therapy in periodontics. Journal of Evidence-Based Dental Practice, 12(3 Suppl.), 50-60.
- Hung, H. C., & Douglass, C. W. (2002). Meta-analysis of the effect of scaling and root planing, surgical treatment and antibiotic therapies. Journal of Clinical Periodontology, 29(11), 975-986.
- Kaldahl, W. B., et al. (1988). Evaluation of four modalities of periodontal therapy. Journal of Periodontology, 59(12), 783-793.
- Kaldahl, W. B., et al. (1996). Long-term evaluation of periodontal therapy: I. Response to 4 therapeutic modalities. Journal of Periodontology, 67(2), 93-102.
- Murphy, K. G., & Gunsolley, J. C. (2003). Guided tissue regeneration for periodontal intrabony and furcation defects. Annals of Periodontology, 8(1), 266-302.
- Preshaw, P. M., et al. (2012). Periodontitis and diabetes: a two-way relationship. Diabetologia, 55(1), 21-31.
- Ramfjord, S. P., & Nissle, R. R. (1974). The modified Widman flap. Journal of Periodontology, 45(8), 601-607.
- Reynolds, M. A., & Aichelmann-Reidy, M. E. (2003). The efficacy of bone replacement grafts in periodontal osseous defects. Annals of Periodontology, 8(1), 227-265.
- Sanz, M., et al. (2020). Treatment of stage I-III periodontitis: the EFP S3 level clinical practice guideline. Journal of Clinical Periodontology, 47(Suppl. 22), 4-60.
- Sculean, A., Nikolidakis, D., & Schwarz, F. (2008). Regeneration of periodontal tissues: barrier membranes and grafting materials. Journal of Clinical Periodontology, 35(8 Suppl.), 106-116.
- Slots, J. (2002). Selection of antimicrobial agents in periodontal therapy. Journal of Periodontal Research, 37(5), 389-398.
- Slots, J., & Jorgensen, M. G. (2002). Effective, safe, practical and affordable periodontal antimicrobial therapy. Periodontology 2000, 28, 298-312.
Questions About Your Periodontal Health?
If you have concerns about your gum health or would like to learn more about any of the topics discussed in this article, we are here to help.