A Note to Our Patients
This guide was written to give you a thorough, honest, and scientifically accurate understanding of periodontal disease. Every statement about disease processes and expected outcomes is supported by peer-reviewed research from the world's leading periodontal journals, the same sources used to train periodontists at the best dental schools.
We believe that informed patients make better decisions and achieve better outcomes. You deserve to understand not just what we recommend, but why we recommend it and what the evidence says about results. That is what this guide provides.
Please bring any questions to your consultation appointment. We are here to help you every step of the way.
You Are Not Alone
If you have been told you have periodontal disease, the first thing we want you to know is this: you are far from alone. National health data shows that nearly half of all American adults over 30, roughly 64.7 million people, have some form of this condition. Among adults 65 and older, that number rises to over 70%. Periodontal disease is one of the most common chronic health conditions in the world, yet it is also one of the most underdiagnosed because it often progresses without obvious pain in its early stages.
The good news? Periodontal disease is both treatable and manageable. Understanding what is happening in your mouth, and why, is the most powerful first step you can take. This guide is written to give you that understanding in clear, honest language, while also providing the scientific depth you deserve as a patient making important decisions about your health.
What Is Periodontal Disease?
Periodontal disease is a chronic inflammatory condition that damages the structures supporting your teeth. Those structures include your gums (gingiva), the ligament that anchors each tooth to the bone (the periodontal ligament), and most importantly, the jawbone (alveolar bone) that holds your teeth in place.
Unlike a cavity, which damages the tooth itself, periodontal disease attacks the foundation your teeth sit in. Think of it this way: a cavity is like damage to the walls of a house, while periodontal disease is like erosion of the foundation beneath it. When enough foundation is lost, even perfectly healthy teeth become loose, shift position, and may eventually need to be removed.
Periodontal disease develops through the interaction of three factors working together: bacteria in your mouth, your body's immune response to those bacteria, and the unique anatomy of your teeth and bone. Let's walk through each one.
The Three Causes of Periodontal Disease
1. Bacteria: The Trigger
Your mouth is home to over 700 species of bacteria and in most people, most of the time, these bacteria live in a balanced community that causes no harm. Problems begin when bacteria are allowed to sit undisturbed on your teeth for extended periods. When this happens, the bacterial community shifts: harmless species are gradually replaced by more aggressive, disease-causing organisms.
These bacteria don't float freely. They organize into a structure called a biofilm, a tightly packed, surface-attached community encased in a protective coating. This biofilm is what you feel as "plaque" on your teeth. The biofilm structure is critically important because it makes the bacteria up to 1,000 times more resistant to antibiotics than free-floating bacteria. This is exactly why antibiotics alone cannot treat periodontal disease; the biofilm must be physically broken up and removed, either during a deep cleaning or through surgery.
As the biofilm matures, the most harmful bacteria become dominant. Researchers have identified a group called the "red complex" (Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola) as the organisms most strongly linked to deep pockets, bleeding gums, and progressive bone loss. Some of these bacteria can actually invade your gum tissue, hiding inside the cells where they are protected from both your immune system and from instruments. This is one of the key reasons we may recommend laser therapy or antibiotics in addition to your deep cleaning, as these treatments can reach bacteria that instruments alone cannot.
Why Can't I Just Take Antibiotics?
The biofilm coating that protects bacteria on your teeth acts like a shield against antibiotics. Until the biofilm is physically broken apart by professional instrumentation (scaling and root planing), antibiotics cannot reach the bacteria effectively. Physical removal is always the first and most critical step in treatment. Antibiotics may be added as a helpful supplement, but never as a substitute for mechanical cleaning.
2. Your Immune System: The Double-Edged Sword
Here is something that surprises many patients: it is not actually the bacteria that directly destroy your bone and gum tissue. It is your body's own immune response to those bacteria that causes most of the damage.
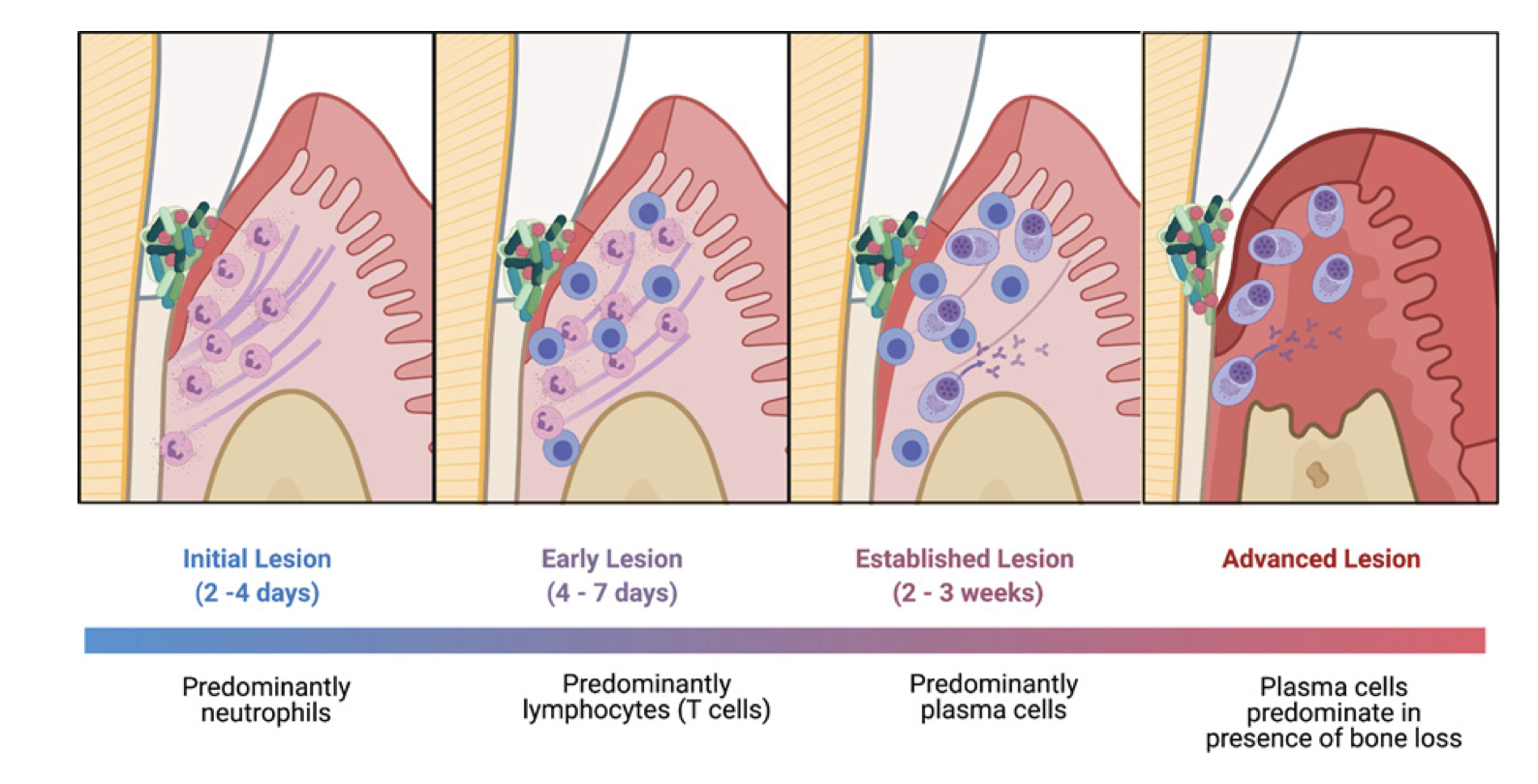
When bacteria build up below your gum line, your immune system detects them and sends defensive cells to fight the infection. If the bacteria are removed quickly, through brushing, flossing, and regular professional cleanings, the immune response resolves and no permanent damage occurs. But when bacteria remain for weeks or months without adequate removal, the immune response becomes chronic. Your body keeps sending inflammatory cells to the area, and these cells release powerful chemicals, including cytokines (IL-1β, IL-6, TNF-α) and enzymes called matrix metalloproteinases, that were designed to fight infection but end up destroying your own bone and connective tissue in the process.
This is the central challenge: your immune system is trying to protect you, but when bacteria persist, that same protective response becomes destructive. Once bone is lost through this process, it does not grow back on its own.
What Affects Your Immune Response?
Some factors are within your control, and some are not. The most important modifiable risk factors are:
- Smoking: The single most damaging modifiable risk factor. Smoking increases harmful bacteria, restricts blood flow to your gums, weakens your immune cells, and impairs the cells (fibroblasts) responsible for tissue repair. Smokers often don't bleed even when disease is active, because nicotine constricts blood vessels, hiding the warning signs.
- Diabetes: Uncontrolled diabetes weakens your immune system, triggers excessive inflammation, and can damage the tiny blood vessels needed for healing. Ideally, your HbA1c should be below 7% for the best treatment outcomes.
- Stress: Chronic stress raises cortisol levels, which suppresses your immune system's ability to fight infection.
Non-modifiable factors include genetic susceptibility, conditions like Down syndrome, and age. The important takeaway: even if you have genetic risk factors, the actions you take (quitting smoking, managing diabetes, practicing excellent oral hygiene) can significantly change the course of your disease.
3. Your Anatomy: The Landscape of Your Mouth
The third factor is the unique anatomy of your teeth and jawbone. Your anatomy influences where bacteria tend to accumulate and what pattern of bone loss develops as disease progresses.
Root grooves: All teeth with multiple roots have grooves running along them. In some patients these grooves are deeper than average, creating sheltered pockets where bacteria hide and accumulate. Premolars can have grooves extending far below the gum line, making them especially challenging to keep clean.
Furcations: This is the area where the roots of a multi-rooted tooth divide. Lower molars have one furcation (two roots); upper molars have three furcations (three roots). When bone loss reaches the furcation, disease spreads through the tooth, not just around it, creating undercuts that trap bacteria and make the area extremely difficult to clean without surgical access.



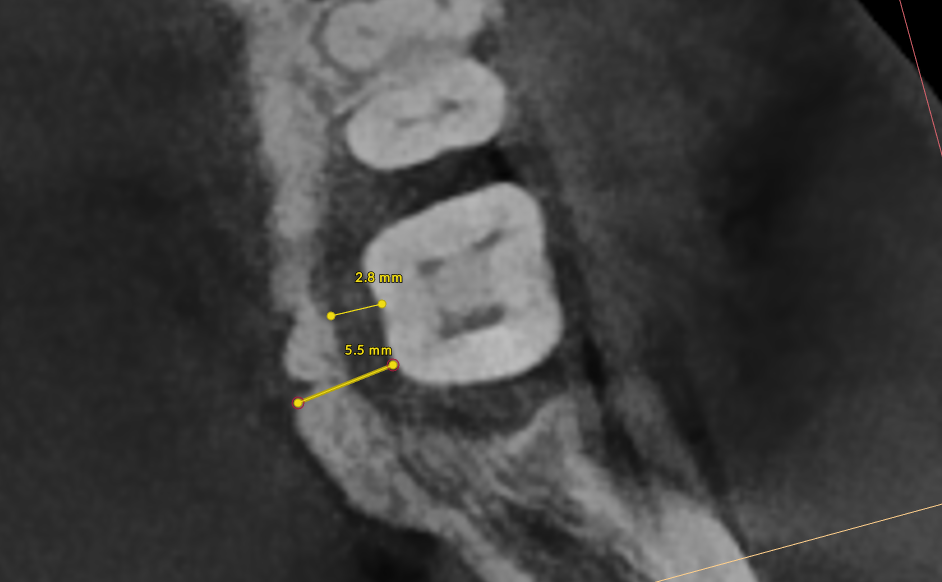
Bone thickness and shape: Bacteria on your teeth can only cause bone destruction within about 1.5 mm of where they sit, referred to as their "sphere of influence." When the surrounding bone is thin or roots are very close together, bacteria can destroy the bone completely, leading to gum recession and more exposed tooth surface. In these cases, non-surgical therapy is often sufficient. When bone is thick, bacteria can only destroy part of it, creating craters or "moats" around the tooth. These craters cannot be fully cleaned with non-surgical treatment and typically require surgery to correct.
How Periodontal Disease Affects Your Life
Effects on Your Mouth
As bone is lost, you may notice teeth feeling looser, teeth shifting position, gaps developing where teeth used to be tight together, food getting stuck in new places, difficulty chewing, and increased sensitivity as root surfaces become exposed. Gum recession can change the appearance of your smile. In advanced cases, painful infections (periodontal abscesses) can develop within deep pockets. Without treatment, the end result is tooth loss.


Effects on Your Overall Health
Research increasingly shows that periodontal disease affects far more than just your mouth. The chronic inflammation it creates contributes to elevated inflammatory markers throughout your body. Studies have found associations between periodontitis and cardiovascular disease (including heart attack and stroke), complications during pregnancy, respiratory infections, rheumatoid arthritis, chronic kidney disease, and even certain cancers. Treating periodontal disease is not just about saving your teeth; it is about protecting your whole-body health.
Effects on Your Daily Life and Confidence
Many patients report feeling self-conscious about their smile, worried about bad breath, embarrassed eating in public, or reluctant to speak closely with others. These feelings are entirely understandable and very common. The psychological stress can actually worsen the disease by suppressing your immune system, creating a cycle that treatment can help break.
How We Diagnose Periodontal Disease
Your periodontal examination involves three key measurements. The current classification system, established by the 2018 World Workshop, categorizes disease by stage (I through IV for severity) and grade (A through C for progression speed).
The Three Key Diagnostic Measurements
- Probing Depths: We gently measure the depth of the space between your gum and each tooth. In health, this pocket measures 1 to 3 mm. At this depth, bacteria can be 100% removed during cleanings and you can keep the area clean at home. Pockets of 4 to 5 mm are "borderline"; we can typically remove about 60 to 70% of bacteria, usually enough to stop bone loss, though these sites need close monitoring. Pockets of 6 mm or deeper are at severe risk, as most bacteria cannot be reached non-surgically.
- Bleeding on Probing: Healthy gums do not bleed. Bleeding during probing tells us active inflammation is present. Important for smokers: nicotine constricts blood vessels, so gums may not bleed even when disease is active.
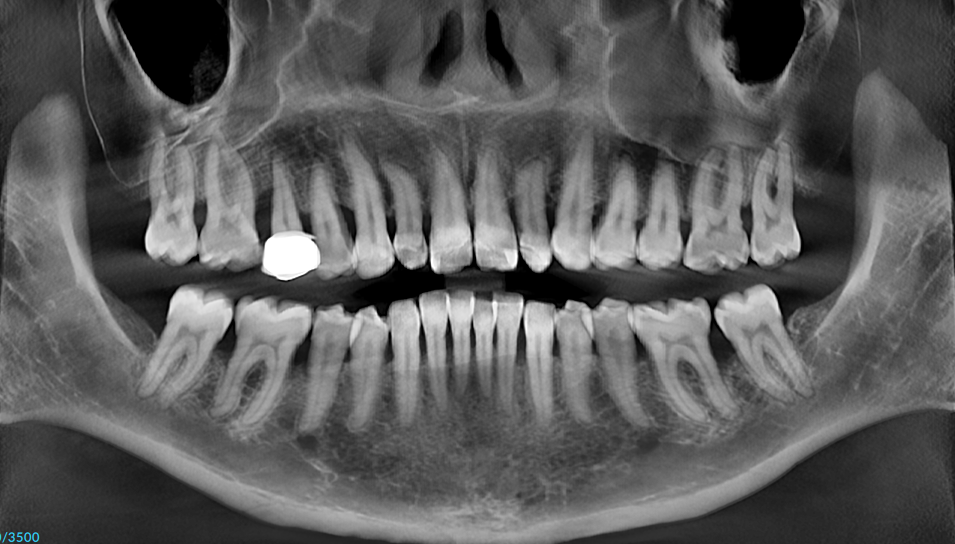
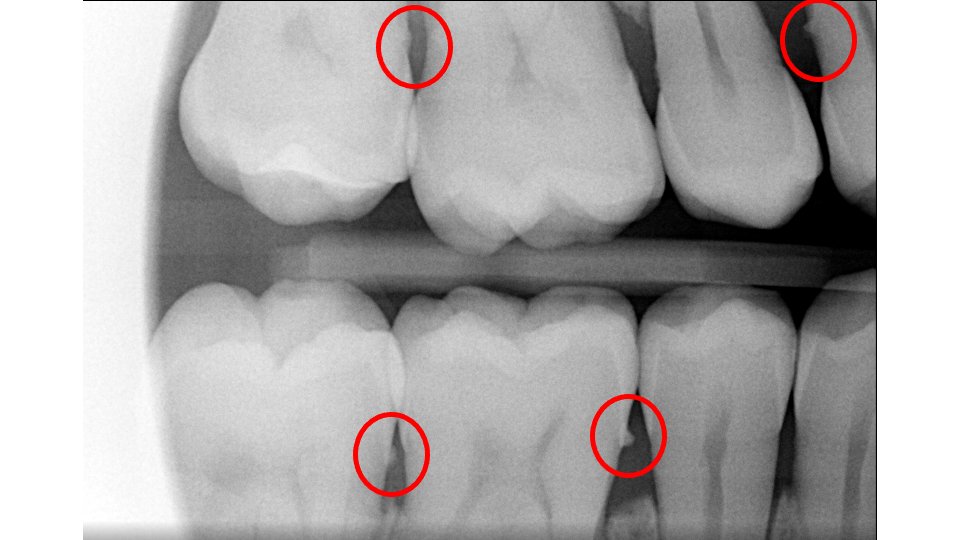
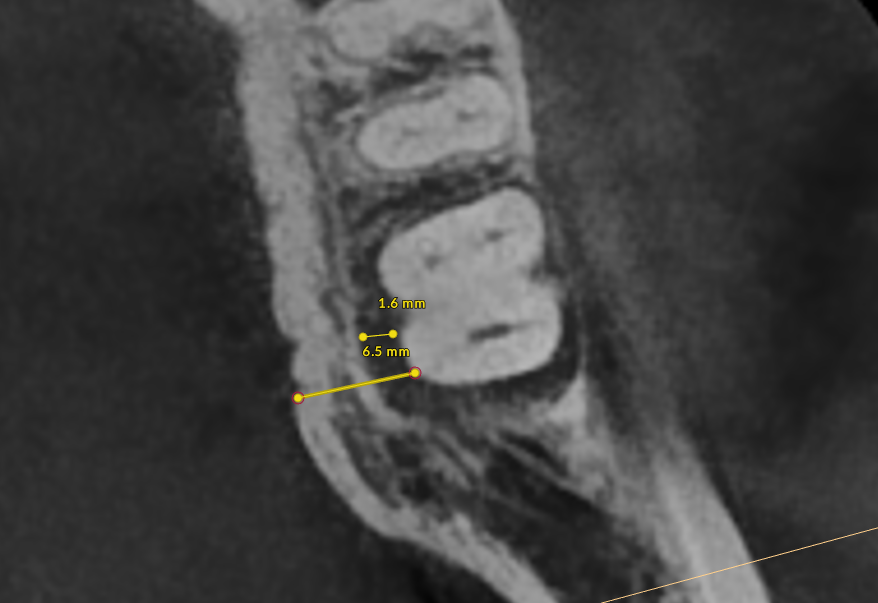
- X-Rays (Radiographs): X-rays show the pattern and extent of bone loss. We can see whether bone has been lost evenly (horizontal loss) or whether craters and vertical defects have formed. This pattern directly determines which type of treatment you need.
The Treatment Pathway: An Overview
Treatment follows a step-by-step approach refined through decades of research and recommended by international guidelines.
Step 1, Oral Hygiene Optimization: The foundation of everything. We will work with you on brushing technique (modified Bass method, soft-bristled brush at the gum line) and the right interdental cleaning tool: floss, water flosser, or interproximal brushes (especially effective when periodontal disease has created wider gaps between teeth).
Step 2, Deep Cleaning (Scaling and Root Planing): The core non-surgical treatment where we remove bacteria, tartar, and toxins from below the gum line under local anesthesia, often with laser therapy and antimicrobial irrigation.
Step 3, Re-Evaluation: Four to eight weeks after deep cleaning, we re-measure every pocket and assess healing.
Step 4, Osseous Surgery (if needed): For pockets that remain deep, surgery gives us direct access to clean root surfaces and reshape or rebuild bone.
Step 5, Lifelong Maintenance: Professional cleanings every three months (sometimes every two) for the rest of your life. Patients who maintain this schedule have excellent long-term outcomes.
The Most Important Message in This Guide
Periodontal disease is treatable and manageable. While we cannot reverse all the damage that has already occurred, we can stop the disease from progressing and, in many cases, rebuild some of what was lost. Patients who commit to treatment and maintenance can keep their teeth for decades. The key is taking action now; the sooner we begin, the more we can preserve.
Ready to Learn About Treatment?
Now that you understand what periodontal disease is and how it affects your oral and overall health, learn about the step-by-step treatment process: Periodontal Treatment: A Complete Guide.
Frequently Asked Questions
Do I have gum disease?
Common signs include gums that bleed when you brush or floss, gums that are red or swollen, persistent bad breath, gums pulling away from your teeth, and teeth that feel loose. If you are experiencing any of these symptoms, ask your dentist to evaluate you for periodontal disease.
What is the difference between gingivitis and periodontitis?
Gingivitis is the earliest stage of gum disease and affects only the gums. It is reversible with proper treatment. Periodontitis is more advanced and involves damage to the bone and connective tissue that support your teeth. Once bone is lost, it does not grow back on its own.
Can gum disease be cured?
Gingivitis can be completely reversed with professional cleaning and improved home care. Periodontitis cannot be cured, but it can be managed and stabilized with proper treatment. The goal of periodontal therapy is to stop the disease from progressing and preserve the teeth and bone you still have.
Is gum disease connected to other health problems?
Yes. Research has linked periodontal disease to heart disease, diabetes, respiratory disease, and complications during pregnancy. The chronic inflammation caused by gum disease can affect your overall health, which is why treatment is important even if you are not in pain.
Why do my gums bleed when I brush my teeth?
Bleeding gums are one of the earliest signs of gum disease. They indicate inflammation caused by bacteria along and below the gum line. Healthy gums should not bleed during normal brushing or flossing. If your gums bleed regularly, you should see a dentist for evaluation.
What happens if I ignore gum disease?
Untreated gum disease progresses over time. Pockets deepen around the teeth, bone is lost, and teeth eventually become loose and may need to be removed. The disease does not resolve on its own and tends to worsen without professional intervention.
Sources
This guide is based on peer-reviewed research published in leading dental and medical journals.
- Bergstrom, J. (2004). Tobacco smoking and chronic destructive periodontal disease. Odontology, 92(1), 1-8.
- Cobb, C. M. (2002). Clinical significance of non-surgical periodontal therapy: an evidence-based perspective of scaling and root planing. Journal of Clinical Periodontology, 29(Suppl. 2), 6-16.
- Darveau, R. P. (2010). Periodontitis: a polymicrobial disruption of host homeostasis. Nature Reviews Microbiology, 8(7), 481-490.
- Eke, P. I., Dye, B. A., Wei, L., et al. (2015). Update on prevalence of periodontitis in adults in the United States: NHANES 2009 to 2012. Journal of Periodontology, 86(5), 611-622.
- Genco, R. J., & Borgnakke, W. S. (2013). Risk factors for periodontal disease. Periodontology 2000, 62(1), 59-94.
- Hajishengallis, G., & Lamont, R. J. (2012). Beyond the red complex and into more complexity: the polymicrobial synergy and dysbiosis (PSD) model. Molecular Oral Microbiology, 27(6), 409-419.
- Papapanou, P. N., Sanz, M., et al. (2018). Periodontitis: consensus report of workgroup 2 of the 2017 World Workshop. Journal of Periodontology, 89(Suppl. 1), S173-S182.
- Preshaw, P. M., Alba, A. L., Herrera, D., et al. (2012). Periodontitis and diabetes: a two-way relationship. Diabetologia, 55(1), 21-31.
- Sanz, M., Herrera, D., Kebschull, M., et al. (2020). Treatment of stage I-III periodontitis: the EFP S3 level clinical practice guideline. Journal of Clinical Periodontology, 47(Suppl. 22), 4-60.
- Socransky, S. S., Haffajee, A. D., Cugini, M. A., Smith, C., & Kent, R. L. Jr. (1998). Microbial complexes in subgingival plaque. Journal of Clinical Periodontology, 25(2), 134-144.
- Tonetti, M. S., Greenwell, H., & Kornman, K. S. (2018). Staging and grading of periodontitis. Journal of Periodontology, 89(Suppl. 1), S159-S172.
Questions About Your Periodontal Health?
If you have concerns about your gum health or would like to learn more about any of the topics discussed in this article, we are here to help.